Good Faith Estimate
Under federal law, you are entitled to receive a “Good Faith Estimate” (GFE) explaining how much your care is expected to cost.
Health care providers must give patients who are uninsured or choosing not to use insurance an estimate of the total expected charges for non-emergency services.
You have the right to receive a Good Faith Estimate for the total expected cost of any non-emergency items or services. This may include fees related to therapy sessions, assessments, or other associated services.
Your provider must give you the Good Faith Estimate in writing at least one business day before your scheduled appointment. You may also request an estimate at any time prior to scheduling services.
If your bill is $400 or more than the Good Faith Estimate, you have the right to dispute the charge.
Be sure to save a copy or photo of your Good Faith Estimate for your records.
For more information about your right to a Good Faith Estimate, visit www.cms.gov/nosurprises or call 800-985-3059.
Beginning January 1, 2022, the federal “No Surprises Act” took effect. This law was created to increase transparency and help clients understand the anticipated costs of their mental health care before beginning services.
At Kindred Counseling, the goal is to provide clear information about session fees and treatment expectations so you can make informed choices about your care.
Because every client’s situation and goals are unique, it is not possible to predict exactly how long therapy will take. Some clients find benefit after a few sessions, while others choose to continue for several months or longer. Frequency and duration often depend on factors such as:
Your goals and reasons for seeking therapy
Progress made toward those goals
Scheduling needs and life circumstances
Therapist availability
Financial considerations
Together, we will periodically review your goals and progress to determine whether therapy should continue, conclude, or shift in focus. You may end therapy at any time.
For ethical, legal, and insurance purposes — and in compliance with the No Surprises Act — a formal diagnosis is required for all clients who receive a Good Faith Estimate. This diagnosis is made following an initial assessment, typically within the first 1–5 sessions.
If you choose to decline a formal diagnosis, Kindred Counseling will not update the Good Faith Estimate. You have the right to make this choice under federal and state guidelines.
Below are some common diagnostic codes that may appear on a Good Faith Estimate. This list is not exhaustive, and your diagnosis may differ based on your clinical assessment:
Adjustment Disorder — F43.23
Unspecified Mental Disorder — F99
Depression, Unspecified — F32.9
Generalized Anxiety Disorder — F41.1
Bipolar Disorder, Unspecified — F31.9
Post-Traumatic Stress Disorder (PTSD) — F43.10
According to the American Psychological Association, research suggests that approximately 15–20 sessions are often needed for about half of clients to experience meaningful improvement. Some clients prefer to engage in longer-term therapy (20–30 sessions or more) to achieve greater stability and maintain progress.
Ultimately, therapy is a collaborative process. We will work together to set goals, track progress, and decide when you feel ready to conclude services. Should your frequency of sessions or treatment plan change, an updated Good Faith Estimate will be provided.
Provider Name: April Williamson, MA, LMFT
Practice Name: Kindred Counseling
License: Minnesota 4668
NPI Number: 1811785645
Phone: 612-412-1384
Location: Telehealth and In Person
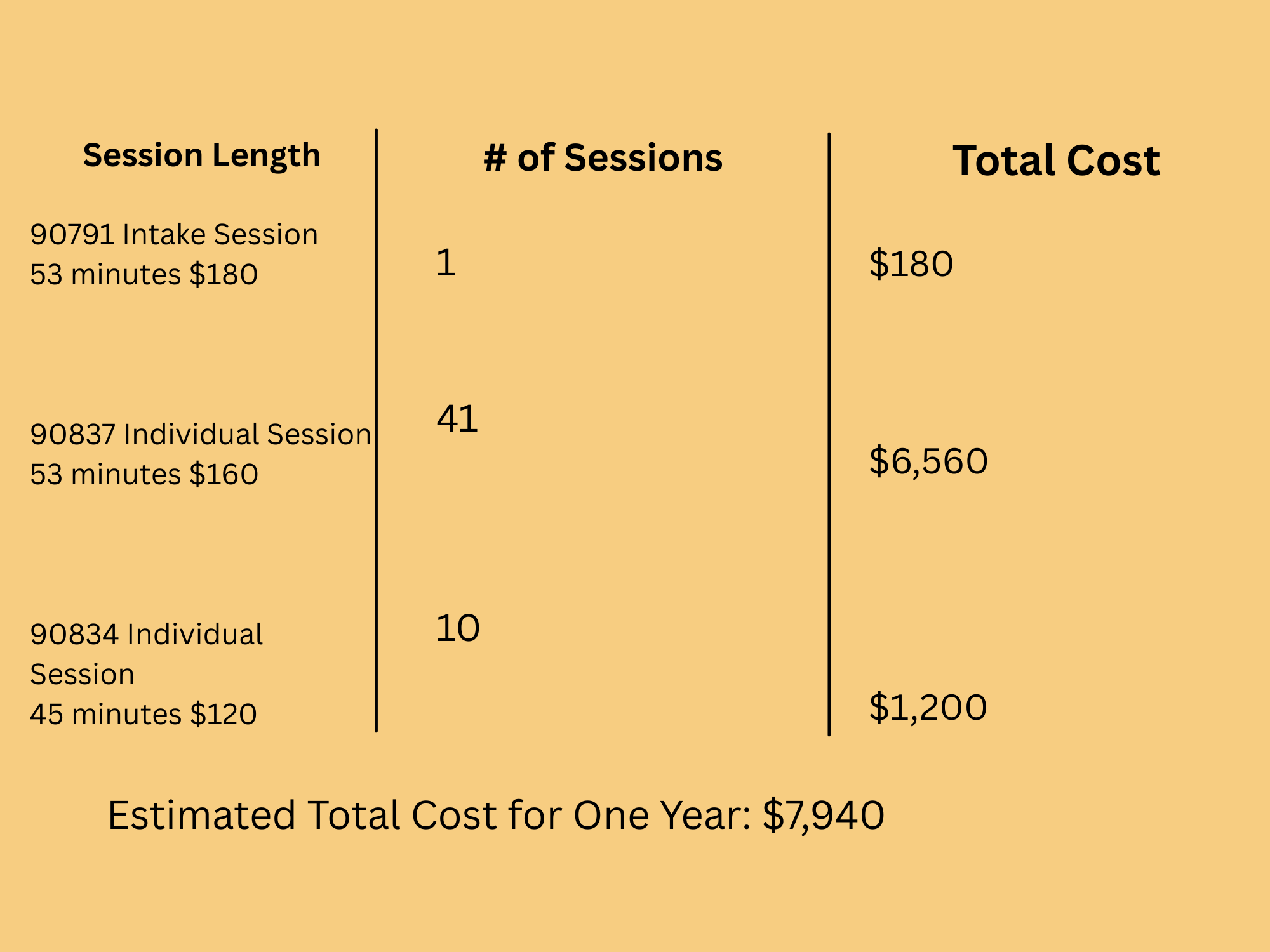
(Note: Costs may vary depending on client needs and frequency of services)
Do you have questions about payments? Please reach out!